Last updated on Aug 5, 2026
Get the free Medical Provider Statement Form
pdfFiller is not affiliated with any government organization
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
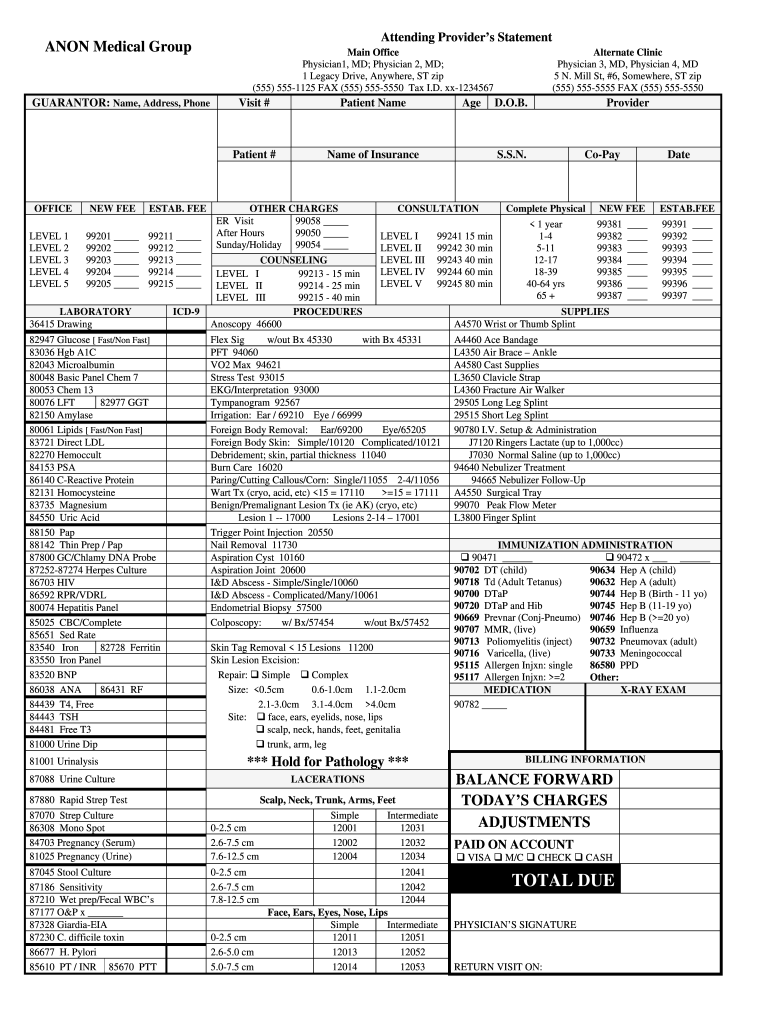
What is ANON Medical Group Attending Providers Statement
The Medical Provider Statement Form is a healthcare document used by healthcare providers to document patient visits, procedures, and billing information.
pdfFiller scores top ratings on review platforms
I enjoy using this product. It's easy to use and send important pdf documents. Great product!
VERY RELIABLE AND EASY TO USE IN EVERYWHERE.
Who needs ANON Medical Group Attending Providers Statement?
Explore how professionals across industries use pdfFiller.

ANON Medical Group Attending Providers Statement is needed by:
-
Healthcare providers documenting patient visits
-
Physicians requiring patient demographic details
-
Billing specialists for insurance processing
-
Medical offices managing patient records
-
Patients needing consent for billing
-
Insurance companies for claim validation
Comprehensive Guide to ANON Medical Group Attending Providers Statement
What is the Medical Provider Statement Form?
The Medical Provider Statement Form is an essential document in healthcare documentation, serving multiple purposes in patient care and billing. This form is designed to capture vital patient information including demographics, insurance details, and medical codes for services rendered. The physician's signature is a critical component, ensuring compliance with billing practices and validating the accuracy of details provided.
-
It facilitates organized documentation for both care and billing, thereby supporting efficient healthcare workflows.
-
Necessary fields within the form allow for comprehensive patient records, essential for effective treatment and insurance processing.
Purpose and Benefits of the Medical Provider Statement Form
This form is crucial for documenting patient visits, which is vital for accurate insurance claims and billing processes. Utilizing a standardized healthcare billing form streamlines patient intake and simplifies billing for healthcare providers. Additionally, it helps maintain organized records that are necessary for legal and compliance purposes in the healthcare field.
-
Clear documentation aids in avoiding billing errors and ensures timely reimbursement from insurers.
-
Facilitates effective communication among healthcare providers, patients, and insurance companies.
Who Needs the Medical Provider Statement Form?
The Medical Provider Statement Form is typically filled out by physicians and healthcare providers during patient visits. It is especially relevant in outpatient clinics and hospitals where accurate documentation of patient information is essential. Patients also benefit by ensuring their medical history and insurance details are recorded correctly for their care.
-
Essential for physicians who must document services rendered accurately for billing.
-
Important for any healthcare professional responsible for patient care and documentation.
How to Fill Out the Medical Provider Statement Form Online
Completing the Medical Provider Statement Form online involves several key steps. First, essential fields such as patient demographics and billing information need to be accurately filled. Utilizing platforms like pdfFiller can simplify this process, making navigation intuitive for users. Avoiding common errors is critical for seamless submission; double-checking information like insurance details can prevent delays.
-
Access the form via pdfFiller and begin filling in all required fields.
-
Review each section for completeness before submitting.
Review and Validation Checklist for the Medical Provider Statement Form
Ensuring accuracy in the Medical Provider Statement Form is vital prior to submission. Completing a thorough checklist can help verify critical details such as signatures, dates, and coding. Double-checking the patient's insurance information and demographic details is essential to avoid common errors.
-
Verify the physician's signature is included.
-
Check that all required fields are correctly filled out.
Submission Methods for the Medical Provider Statement Form
Submitting the completed Medical Provider Statement Form can be accomplished through various methods. Methods include e-filing, mailing, or submitting in person, depending on the healthcare system or insurer's requirements. Understanding applicable fees and deadlines is crucial to ensure timely processing.
-
E-filing for quick and efficient submission.
-
Direct mail to specific healthcare providers or insurers as required.
What Happens After You Submit the Medical Provider Statement Form?
After submitting the form, it typically undergoes a processing period where claims are reviewed. Users should know how to follow up or track the submission status through their insurance providers or healthcare systems. Being aware of common reasons for rejection can provide guidance on steps for correction if necessary.
-
Understand the typical processing timeline for your submission.
-
Know how to contact your provider for status updates.
Why Choose pdfFiller for the Medical Provider Statement Form?
pdfFiller stands out as a preferred solution for managing the Medical Provider Statement Form. It offers key features that facilitate a secure and efficient online process for completing, signing, and managing healthcare forms. The platform is compliant with HIPAA standards, ensuring the security of sensitive healthcare information.
-
Advanced document management capabilities for ease of use.
-
Robust security measures to protect patient information.
Get Started with the Medical Provider Statement Form Today
Utilizing pdfFiller simplifies the process of filling and signing the Medical Provider Statement Form. With cloud technology, users can access and store their forms securely, enhancing overall document management. Trying pdfFiller for your healthcare documentation needs offers a seamless experience in managing essential forms.
-
Begin filling out your form with straightforward online tools.
-
Experience enhanced security for sensitive healthcare documents.
How to fill out the ANON Medical Group Attending Providers Statement
-
1.To access the Medical Provider Statement Form on pdfFiller, navigate to the pdfFiller website and use the search bar to locate the form.
-
2.Once you open the form, familiarize yourself with the layout including sections for patient information, insurance details, and medical codes.
-
3.Before you begin filling out the form, gather all necessary information, such as patient demographics, insurance policy numbers, and details of medical services provided.
-
4.Click on each field to enter the required information. pdfFiller allows you to type directly into the form fields, ensuring easy data entry.
-
5.For patient demographics, enter the patient's name, date of birth, and contact information. Ensure accuracy as this information is crucial for billing and insurance claims.
-
6.Fill out the insurance details section, providing the name of the insurance company, policy number, and any necessary group information.
-
7.In the services rendered section, include the medical codes for each service provided. Refer to coding guidelines if necessary.
-
8.Review each section of the form to ensure all information is complete and correct. Pay special attention to the signature line for the physician.
-
9.Once all fields are accurately filled, save your work on pdfFiller. You can download the completed form or submit it directly through the platform, based on your processing needs.
Who needs to fill out the Medical Provider Statement Form?
Healthcare providers, particularly physicians, need to complete this form to document patient visits and services rendered for billing and insurance claims.
What is the main purpose of the Medical Provider Statement Form?
The primary purpose of this form is to provide comprehensive documentation of patient visits, procedures, and billing information necessary for insurance reimbursements.
Is notarization required for this form?
No, the Medical Provider Statement Form does not require notarizing. It requires the physician's signature but not notarization.
What information is necessary to fill out the form correctly?
To complete the form accurately, gather patient demographics, insurance details, and medical codes for services provided during the visit.
How can I submit the completed form?
You can save the completed Medical Provider Statement Form as a PDF and submit it electronically to the relevant insurance company or save it for your records.
What common mistakes should I avoid?
Ensure all fields are filled in correctly and completely. Missing patient information or incorrect medical codes can delay billing and insurance processing.
What are the processing times for this form?
Processing times can vary based on the insurance provider's requirements. Typically, allow 2-4 weeks for claims processing once submitted.
Related Content
Related Forms


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.